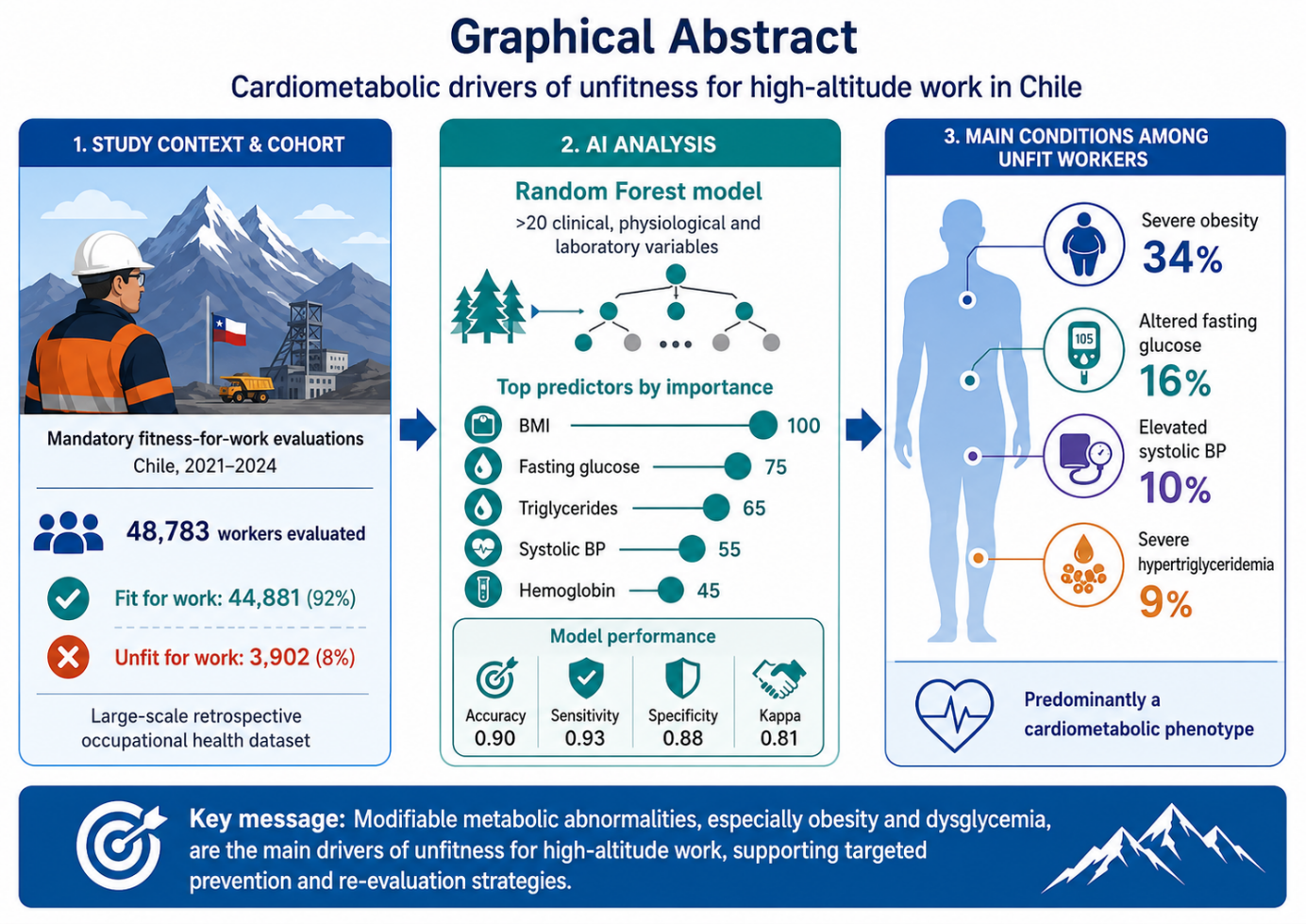
Workers exposed to chronic intermittent hypobaric hypoxia at high altitude (HA) face substantial cardiometabolic demands that may compromise occupational safety. Fitness-for-work (FFW) assessments are routinely performed in Chile under nationally standardized guidelines, yet the internal structure of the unfit population and codependence among predictive biomarkers remain poorly characterized. This retrospective study analyzed 48,783 workers undergoing mandatory pre-employment FFW evaluations for HA exposure in Chile (2021–2024), of whom 8% were classified as unfit for work (UFW). A supervised Random Forest model, applied to more than 20 clinical, physiological, and laboratory variables, identified key predictors of FFW classification by capturing nonlinear interactions among variables that univariate approaches cannot detect. The model achieved precision 0.90 (95% CI: 0.89–0.92), sensitivity 0.93, specificity 0.88, and kappa 0.807. Body mass index was the most influential predictor, followed by fasting plasma glucose, triglycerides, and systolic blood pressure. Among unfit workers, severe obesity (BMI ≥ 35 kg/m2) was the most prevalent condition (34%), followed by altered fasting glucose (16%), elevated systolic blood pressure (10%), and severe hypertriglyceridemia (9%). The unfit population was predominantly male with age-related distribution. These findings reveal a cardiometabolic pattern as the dominant driver of HA occupational unfitness. Targeted strategies addressing obesity, glycemia, and dyslipidemia, alongside risk-based monitoring aligned with Chile’s national standards, may reduce exclusion rates and support more individualized FFW evaluations in HA settings. Aim: to characterize dominant cardiometabolic patterns in workers classified as unfit for HA occupational exposure in Chile and to quantify their relative weight using a Random Forest variable-importance framework. Methods: retrospective analysis of 48,783 pre-employment FFW evaluations (2021–2024) from a national occupational-health surveillance system; supervised Random Forest model with stratified 70/30 train-test split and repeated 10-fold cross-validation. Conclusion: targeted preventive strategies focused on obesity, glycemia, and dyslipidemia, combined with structured re-evaluation pathways, could reduce HA occupational exclusion and inform the future refinement of FFW criteria.
- Open Access
- Article
Cardiometabolic Pattern of Workers Unfit for High-Altitude Occupational Exposure in Chile: A Large-Scale Retrospective Analysis Using a Random Forest Model ‡
- Ricardo Jorquera 1,
- Guillermo Droppelmann 2,*,†,
- Gonzalo Blanco 1,
- Max Dollmann 1,
- Ignacio Ahumada 1,
- Felipe Feijoo 3,†
Author Information
Received: 14 Apr 2026 | Revised: 20 May 2026 | Accepted: 05 Jun 2026 | Published: 18 Jun 2026
Abstract
Graphical Abstract
Keywords
artificial intelligence | biomarkers | cardiovascular risk | fitness-for-work | hypobaric hypoxia | occupational medicine | random forest
References
- 1.
Luks, A.M.; Swenson, E.R.; Bärtsch, P. Acute high-altitude sickness. Eur. Respir. Rev. 2017, 26, 160096. https://doi.org/10.1183/16000617.0096-2016.
- 2.
Mallet, R.T.; Burtscher, J.; Richalet, J.-P.; et al. Impact of high altitude on cardiovascular health: Current perspectives. Vasc. Health Risk Manag. 2021, 17, 317–335. https://doi.org/10.2147/VHRM.S294121.
- 3.
Aragón-Vela, J.; Bejder, J.; Huertas, R.J.; et al. Does intermittent exposure to high altitude increase the risk of cardiovascular disease in workers? A systematic narrative review. BMJ Open. 2020, 10, e041532. https://doi.org/10.1136/bmjopen-2020-041532.
- 4.
Palmer, K.T.; Cox, R.A.; Brown, I. Fitness for Work: The Medical Aspects; Oxford University Press: Oxford, UK, 2007.
- 5.
Ministerio de Salud de Chile. Guía Técnica: Exposición a Hipobaria Intermitente Crónica. (In Spanish). Available online: https://www.minsal.cl/sites/default/files/guia_hipobaria_altitud.pdf (accessed on 14 April 2026).
- 6.
Superintendencia de Seguridad Social. Compendio de Normas del Seguro Social. Available online: https://www.suseso.gob.cl/613/w3-propertyname-647.html (accessed on 14 April 2026).
- 7.
Serra, C.; Rodriguez, M.C.; Delclos, G.L.; et al. Criteria and methods used for the assessment of fitness for work: A systematic review. Occup. Environ. Med. 2007, 64, 304–312. https://doi.org/10.1136/oem.2006.029397.
- 8.
Vinnikov, D.; Krasotski, V. Healthy worker survival effect at a high-altitude mine. Sci. Rep. 2022, 12, 13903. https://doi.org/10.1038/s41598-022-18331-4.
- 9.
Sarkar, S.; Maiti, J. Machine learning in occupational accident analysis: A review using science mapping approach with citation network analysis. Saf. Sci. 2020, 121, 104900. https://doi.org/10.1016/j.ssci.2020.104900.
- 10.
Vandersmissen, G.J.; Schouteden, M.; Verbeek, C.; et al. Prevalence of high cardiovascular risk by economic sector. Int. Arch. Occup. Environ. Health 2020, 93, 843–853. https://doi.org/10.1007/s00420-019-01458-9.
- 11.
Muñoz, S.; Nazzal, C.; Jimenez, D.; et al. Health effects of chronic intermittent hypoxia among Chilean miners: Rationale, design, and baseline results of a longitudinal study. Ann. Work Expo. Health 2021, 65, 908–918. https://doi.org/10.1093/annweh/wxab029.
- 12.
Vinnikov, D.; Saktapov, A.; Romanova, Z.; et al. Work at high altitude and non-fatal cardiovascular disease associated with unfitness to work. PLoS ONE 2024, 19, e0306046. https://doi.org/10.1371/journal.pone.0306046.
- 13.
Carrillo, J.; Mahecha-Matsudo, S.; Droppelmann, G.; et al. Riesgo de apnea obstructiva del sueño y nivel de actividad física y su asociación con riesgo cardiovascular elevado en adultos chilenos. Rev. Chil. Enferm. Respir. 2019, 35, 22–30. https://doi.org/10.4067/S0717-73482019000100022.
- 14.
Jorquera, R.; Droppelmann, G.; Blanco, G.; et al. Data-driven identification of metabolic and cardiovascular biomarkers in high-altitude workers: A machine learning approach. Front. Public Health 2025, 13, 1652605. https://doi.org/10.3389/fpubh.2025.1652605.
- 15.
Jorquera, R.; Droppelmann, G.; Dollmann, M.; et al. Mining the risk: Early cardiovascular detection in workers. Front. Med. 2025, 12, 1678172. https://doi.org/10.3389/fmed.2025.1678172.
- 16.
Esenamanova, M.K.; Kochkorova, F.A.; Tsivinskaya, T.A.; et al. Chronic intermittent high altitude exposure, occupation, and body mass index in workers of mining industry. High Alt. Med. Biol. 2014, 15, 412–417. https://doi.org/10.1089/ham.2013.1150.
- 17.
Montes-Madariaga, E.S.; Ortiz-Saavedra, B.; Mamani-Castillo, J.S.; et al. Cardiovascular risk and obesity in miner workers exposed to intermittent hypobaric hypoxia in the Peruvian Andes. Front. Physiol. 2026, 17, 1693470. https://doi.org/10.3389/fphys.2026.1693470.
- 18.
Noubiap, J.J.; Nansseu, J.R.; Nyaga, U.F.; et al. Worldwide trends in metabolic syndrome from 2000 to 2023: A systematic review and modelling analysis. Nat Commun. 2025, 17, 573. doi: 10.1038/s41467-025-67268-5.
- 19.
Parra-Gómez, L.A.; Rojas, J.P.; Vásquez, A.J.; et al. Prevalence of metabolic syndrome in Latin America: A systematic review and meta-analysis of observational studies. Diabetes Metab. Syndr. Clin. Res. Rev. 2025, 19, 103282. https://doi.org/10.1016/j.dsx.2025.103282.
- 20.
Zila-Velasque, J.P.; Grados-Espinoza, P.; Challapa-Mamani, M.R.; et al. Prevalence of metabolic syndrome and its Donecomponents according to altitude levels: A systematic review and meta-analysis. Sci. Rep. 2024, 14, 77928. https://doi.org/10.1038/s41598-024-77928-z.
- 21.
Cappelli, F.; Castronuovo, G.; Grimaldi, S.; et al. Random Forest and feature importance measures for discriminating the most influential environmental factors in predicting cardiovascular and respiratory diseases. Int. J. Environ. Res. Public Health 2024, 21, 867. https://doi.org/10.3390/ijerph21070867.
- 22.
Liu, T.; Krentz, A.; Lu, L.; et al. Machine learning based prediction models for cardiovascular disease risk using electronic health records data: Systematic review and meta-analysis. Eur Heart J Digit Health 2024, 6, 7–22. https://doi.org/10.1093/ehjdh/ztae080.
- 23.
Burtscher, M.; Ponchia, A. The risk of cardiovascular events during leisure time activities at altitude. Prog. Cardiovasc. Dis. 2010, 52, 507–511. https://doi.org/10.1016/j.pcad.2010.02.008.
- 24.
Richalet, J.-P.; Hermand, E.; Lhuissier, F.J. Cardiovascular physiology and pathophysiology at high altitude. Nat. Rev. Cardiol. 2024, 21, 75–88. https://doi.org/10.1038/s41569-023-00924-9.

This work is licensed under a Creative Commons Attribution 4.0 International License.
 Suite 4002 Level 4, 447 Collins Street, Melbourne, Victoria 3000, Australia
Suite 4002 Level 4, 447 Collins Street, Melbourne, Victoria 3000, Australia General Inquiries: info@sciltp.com
General Inquiries: info@sciltp.com